HIV/AIDS and Heroin: Where Is NJ's Leadership?
Topic: COMMUNITY INTEREST
HIV/AIDS and Heroin: Where Is NJ's Leadership?
By Tammy Duffy
There are 565 municipalities in the State of New Jersey. The township of Hamilton, Mercer County, ranks 75th in the state of NJ for the highest number of new HIV/AIDS cases.

Source:
http://www.state.nj.us/health/aids/repa/topcity/documents/topcity.pdf
This should come to no surprise for as reported in March 2015, it was presented by Duffy's Cultural Couture,
(http://www.tammyduffy.com/ARTFASHION/index.blog?entry_id=2352388)
that Hamilton Township, Mercer county, ranks 26th in the state for residents admitted to drug treatment during for heroin and other opiates. (Source: NJ Dept of Human Services, 121 Hamilton residents were admitted in 2013). There is a correlation. What is the leadership of Hamilton doing about these two glaring public health issues?
Let's look away from Hamilton and look at what is happening in Indiana. The leadership in Scott County, Indiana learned the hard way that there is a correlation between AIDS and heroin use.
So far, the Indiana State Department of Health has confirmed more than 150 people have been diagnosed with new cases of HIV. There are 125 cases in Hamilton township. NJ, not far behind. The vast majority of cases are in Scott County, Indiana – most linked to Austin – where the disease has spread rapidly among intravenous drug users who share dirty needles. This was happening and the town had no idea.
Through a series of interviews and public information requests, the local Indiana Channel 13 investigated and assembled a detailed timeline of the epidemic. It reveals a breakdown in communication between officials at the state and local level which, some healthcare experts say, prevented a more timely warning to residents and healthcare workers who were unaware of a developing crisis in their own backyard. This can happen in Hamilton, Mercer County. It is happening and the towns leadership has chosen to ignore it.
The residents have seen this exact behavior on more than one occasion by the leadership and health department in Hamilton NJ. Confusion, unclear direction and a blatant disregard for public safety and health. Several months ago in the township of Hamilton there was the first death from EV D68. Several months prior to this death, there was a nation wide epidemic occurring. While this was occurring there was zero communication until the death of a resident. There was zero proactive measures taken (like seen in surrounding towns like Princeton) to safeguard the community and stop a tragedy like the death of a small boy, from happening. In this same town there have been 12 narcon deployments, the last of which resulted in the death of a resident, and the leadership in Hamilton is quiet as a church mouse. Let's not forget to mention the rejection of the changes to the restaurant inspections fines. Why is that? Why did the leadership of Hamilton repeatedly say in the press conferences after the EVD68 death of the resident," When I went to the schools and said does anyone know what EV D 68 is?" The mayor said," No one knew." Who's fault is it that no one knew? I would say it is 100% her fault that no one knew. It is the fault of her leadership and the Health Department. A child died. A parent should never have to bury their child. The leadership in towns need to be held accountable for these deaths and blatant disregard to the public health of the residents.
One of the greatest ironies of the Scott County HIV outbreak is the location of the county's health department. The health department shares a parking lot with the county hospital, where the outbreak's earliest HIV cases were diagnosed back in December. In fact, the front door of the Scott County Health Department is just 45 steps from the front door of the hospital. Why did it take two months for critical information to make its way across a parking? Probably the same reason that residents in Hamilton are not getting educated on HIV/AID and Heroin. The same reason no one was educated on EVD68 until there was a death, etc. There is no other explanation other than abysmal leadership.
The state of NJ ranks 5th in the nation as it pertains to newly diagnosed cases of HIV/AID. There were 54,557 new cases in 2014, (801 Diagnosed under the age of 13). Even though New Jersey is one of the smaller states in the United States it has a higher HIV/AIDS rate. This makes Jersey’s ratio higher than any other state in the country. One can only question why any political leadership in NJ would continue to ignore these very important public health issues.
What are the Numbers on HIV/AIDS in NJ
NEW JERSEY: 75,200 cumulative HIV/AIDS cases; 35,688 current cases living with HIV/AIDS
MERCER COUNTY: 2,519 cumulative HIV/AIDS cases; 1,356 current cases living with HIV/AIDS
• Minorities account for 76 percent of the cumulative adult/adolescent HIV/AIDS cases.
• Thirty-five percent of those living with HIV/ AIDS are females.
• Seventy-nine percent of those living with HIV or AIDS are 40 years of age or older.
• Recently reported cases of adult/adolescent HIV and AIDS are older at diagnosis than previously reported cases.
| Statewide Summary:
Prevalence of Persons Currently Living with HIV/AIDS in NJ |
| Persons Living with HIV/AIDS | 38,075 |
| Total Population, Estimate 7/1/2013 | 8,899,339 |
| Prevalence Rate per 100,000 population | 427.82 |
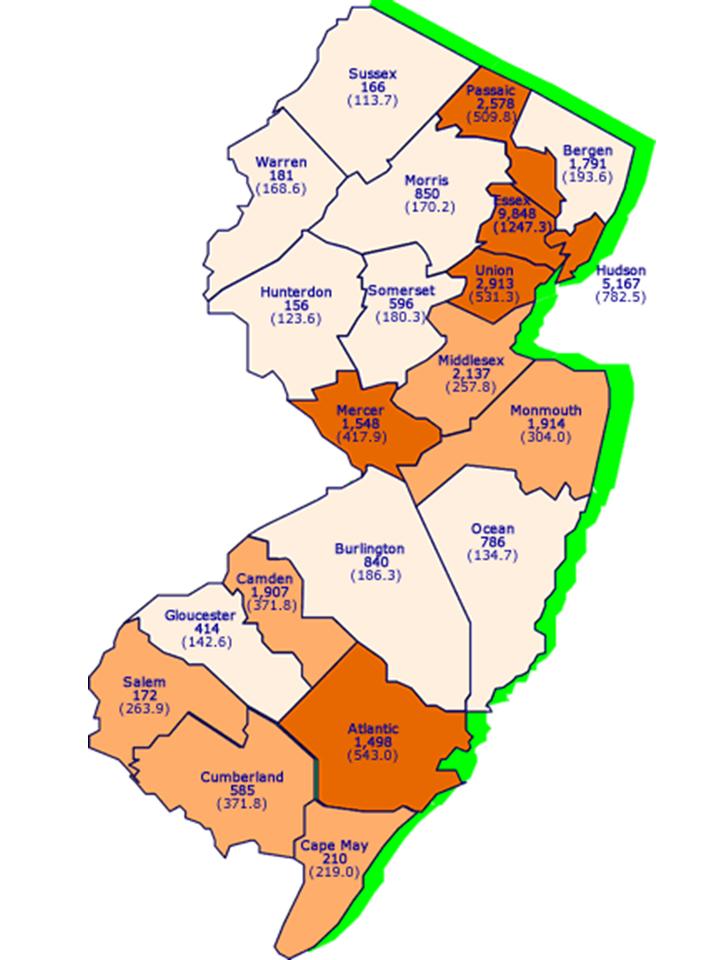
| Prevalence Rate: Persons Living with HIV/AIDS per 100,000 population |
| | 0.0 - 199.9 |
| | 200.0 - 399.9 |
| | 400.0 - 1299.9 |
| Cases not on map | # |
| County Unknown | 13 |
| Incarcerated at
Diagnosis | 1,805 |
Prevalence Rate by County of
Persons Living with HIV/AIDS
Reported as of December 31, 2014
| Mercer County Adult/Adolescent HIV/AIDS Cases |
| |
| | Age Group Data - Mercer County | | | | Known Age at Diagnosis | Males | Females | Totals | | | No. | % | No. | % | No. | % | | | | | | | | | | <13 | 20 | # | 20 | # | 40 | # | | 13-24 | 120 | 7% | 74 | 9% | 194 | 8% | | 25-34 | 479 | 29% | 277 | 35% | 756 | 31% | | 35-44 | 611 | 37% | 255 | 33% | 866 | 36% | | 45-54 | 289 | 18% | 104 | 13% | 393 | 16% | | >=55 | 122 | 7% | 51 | 7% | 173 | 7% | | | | | | | | | | Total | 1,641 | | 781 | | 2,422 | | | | | | | | | | | Race/Ethnicity - Mercer County | | | | Adults/ Adolescents (2) | Males | Females | Totals | | | No. | % | No. | % | No. | % | | | | | | | | | | Hispanic, All races | 210 | 13% | 70 | 9% | 280 | 12% | | Not Hispanic, Black or African America | 1,030 | 63% | 604 | 77% | 1,634 | 67% | | Not Hispanic, White | 389 | 24% | 103 | 13% | 492 | 20% | | Other/Unknown | 12 | # | # | # | 16 | # | | | | | | | | | | Total | 1,641 | | 781 | | 2,422 | | | | | | | | | |
In 2015, it's estimated that the reported cases of HIV could be 621.75% higher than the reported number of cases of syphilis in the greater Jersey City area.
More than 1.2 million people in the United States are living with HIV infection, and almost 1 in 7 (14%) are unaware of their infection. Gay, bisexual, and other men who have sex with men (MSM), particularly young black/African American MSM, are most seriously affected by HIV.
By race, blacks/African Americans face the most severe burden of HIV. The CDC estimates that 1,201,100 persons aged 13 years and older are living with HIV infection, including 168,300 (14%) who are unaware of their infection. Over the past decade, the number of people living with HIV has increased, while the annual number of new HIV infections has remained relatively stable. Still, the pace of new infections continues at far too high a level—particularly among certain groups.
HIV Incidence (new infections): The estimated incidence of HIV has remained stable overall in recent years, at about 50,000 new HIV infections per year. Within the overall estimates, however, some groups are affected more than others. MSM continue to bear the greatest burden of HIV infection, and among races/ethnicities, African Americans continue to be disproportionately affected.
HIV Diagnoses (new diagnoses, regardless of when infection occurred or stage of disease at diagnosis): In 2013, an estimated 47,352 people were diagnosed with HIV infection in the United States. In that same year, an estimated 26,688 people were diagnosed with AIDS. Overall, an estimated 1,194,039 people in the United States have been diagnosed with AIDS.
Deaths: An estimated 13,712 people with an AIDS diagnosis died in 2012, and approximately 658,507 people in the United States with an AIDS diagnosis have died overall. The deaths of persons with an AIDS diagnosis can be due to any cause—that is, the death may or may not be related to AIDS.
Since the epidemic began, almost 92,613 persons with AIDS that were infected through heterosexual sex, have died, including an estimated 4,550 in 2012.
New HIV infections among women are primarily attributed to heterosexual contact (84% in 2010) or injection drug use (16% in 2010). Women accounted for 20% of estimated new HIV infections in 2010 and 23% of those living with HIV infection in 2011. The 9,500 new infections among women in 2010 reflect a significant 21% decrease from the 12,000 new infections that occurred among this group in 2008.
Injection drug users represented 8% of new HIV infections in 2010 and 15% of those living with HIV in 2011. Since the epidemic began, nearly 186,728 people with (AIDS) who inject drugs have died, including an estimated 3,514 in 2012.
In FY 2014, U.S. federal funding to combat HIV totaled $29.5 billion. Of this, 55% was for care, 10% for cash and housing assistance, 9% for research, 3% for prevention, and 22% for the global epidemic.
Key programs that provide health insurance coverage, care, and support to people with HIV in the U.S. include Medicaid, Medicare, the Ryan White Program, and HOPWA, the Housing Opportunities for Persons with HIV/AIDS Program. Social Security’s income programs for those who are disabled (SSI and SSDI) are also important sources of support.
A variety of federally and state-supported prevention services are provided by state and local health departments and community organizations.
The passage of the Affordable Care Act in March 2010 provides new opportunities for expanding health care access, prevention, and treatment services for millions of people in the U.S., including many people with or at risk for HIV.
In July 2010, the U.S. government released the National HIV/AIDS Strategy, the first comprehensive plan for addressing the epidemic in the U.S. The strategy has three primary goals: reduce new HIV infections; increase access to care and improve health outcomes; and reduce HIV-related health disparities. To further address these, President Obama issued an Executive Order to establish an HIV Care Continuum Initiative in July 2013, and the Administration has begun to outline recommendations, develop action steps, and mark progress toward the goals set forth in the Initiative.
The money and programs are there to help people. The federal budget request for fiscal year (FY) 2015 included a total of $30.4 billion for domestic HIV and AIDS, a 2.3 percent increase from the FY 2014 funding, which totaled $29.7 billion. Of this, 57 percent is for care and treatment, 9 percent for research, 10 percent for cash and housing assistance, and 3 percent for prevention.
AIDS in the United States
New AIDS diagnoses: At the end of 2010, the South accounted for 45% of the estimated 33,015 new AIDS diagnoses in the 50 states and the District of Columbia, followed by the Northeast (24%), the West (19%), and the Midwest (13%).
Since 2010, the Northeast reported the highest rate of new AIDS diagnoses (14.2/100,000), followed by the South (13.0/100,000), the West (8.8/100,000), and the Midwest (6.3/100,000).
Living with an AIDS diagnosis: In 2009, the South accounted for 40% of the estimated 476,732 persons living with an AIDS diagnosis in the 50 states and the District of Columbia, followed by the Northeast (29%), the West (20%), and the Midwest (11%).
In 2009, the Northeast reported the highest rate of persons per 100,000 population living with an AIDS diagnosis (248.7/100,000), followed by the South (169.5/100,000), the West (133.6/100,000), and the Midwest (77.2/100,000).
AIDS deaths: In 2009, the South accounted for 48% of the 17,774 persons with a diagnosis of AIDS who died in the 50 states and the District of Columbia, followed by the Northeast (24%), the West (17%), and the Midwest (11%).
That same year, the Northeast reported the highest rate of deaths of persons with AIDS (7.7/100,000), followed by the South (7.6/100,000), the West (4.2/100,000), and the Midwest (2.8/100,000).
Deaths of persons with an AIDS diagnosis may be due to any cause. The HIV epidemic in Indiana is real. But the real epidemic is the opiate addiction among the citizens of Scott County. The HIV outbreak is a direct result of the addiction epidemic. You can make available all the new needles with needle program but unless you do something about the main issue of the addiction epidemic, this is only a temporary solution. Treat the addict, make adequate addiction help affordable and available, make suboxone treatment available, get addiction counselors into the area, set up mental health programs and outreach programs to the addict and their families. Towns need to quit treating opiate addiction as if it is a big fat secret that no one wants to admit is happening. The idea that a junkie is some homeless uneducated worthless person is the farthest from the truth. The political leadership in towns need to wake up. The towns leadership had an employee ( http://www.nj.com/mercer/index.ssf/2014/09/hamilton_township_employee_arrested_on_drug_charges.html) under their own noses who was charged with intent to distribute drugs. Do you think taxpayers of Hamilton are still paying this employees salary?
The addicts are every day people, your neighbor, your soccer mom, your teenager, your professionals, it's non discriminatory. Leaders and people need to stop the judgments and start the treatments. Get to the source of the epidemic and treat the cause. Way too many lives are lost or forever changed due to the effects of opiate addiction and this needs to change. I believe most addicts want help but have no resources readily available to them or are afraid of being judged or socially scorned. The residents are afraid that their confidentiality will be ignored. During a recent hepatitis clinic, Hamilton township officials allowed camera crews to enter, ignoring the confidentiality of all those who attended. The patients who attended the clinic found themselves on the national news that evening. A massive HIPAA violation.
This being said, we as a society need to quit looking the other way and address this issue head on. The leaderships in towns that chose to ignore these issues should be charged with crimes. They are in a position of power to make a difference. When they choose not to and ignore it, they represent a very stupid part of society.
Sources
CDC. Monitoring selected national HIV prevention and care objectives by using HIV surveillance data—United States and 6 dependent areas—2012. HIV Surveillance Supplemental Report 2014;19(No.3). Published November 2014.
2CDC. Estimated HIV incidence in the United States, 2007–2010. HIV Surveillance Supplemental Report 2012;17(No. 4). Published December 2012.
3CDC. HIV Surveillance Report,2013; vol. 25. Published February 2015.
4Purcell D, Johnson CH, Lansky A, et al. Estimating the population size of men who have sex with men in the United States to obtain HIV and syphilis rates. Open AIDS Journal 2012;6 (Suppl 1: M6): 98-107.
5CDC. Estimated lifetime risk for diagnosis of HIV infection among Hispanics/Latinos— 37 states and Puerto Rico, 2007. MMWR 2010:59 (40);1297-1301.
Additional Resources
Posted by tammyduffy
at 12:01 AM EDT
Updated: Sunday, 24 May 2015 4:59 PM EDT

 Edward Hopper, Universalist Church, 1926. Watercolor over graphite on cream wove paper. Laura P. Hall Memorial CollectionThe works in the exhibition address broad artistic and historical trends while revealing the medium’s distinctive technical properties as an amalgam of painting and drawing. They also represent a wide range of subject matter and styles. Highlights include Winslow Homer’s Eastern Point Light (1880), an evocative portrayal of two ships, one brilliantly silhouetted by moonlight;Universalist Church (1926) by Edward Hopper, a dramatically cropped study of New England light on a historic church steeple and the structures that surround it; and Jacob Lawrence’s The Workshop (1978), whose signature flattened colors embody the artist’s modernist sensibility. Landscape plays a major role in the medium, as seen in such images as the dramatic mountain scene (ca. 1908) by John Singer Sargent, Arthur Dove’s interlocking Two Trees (1937), and the swirling forms and life-affirming spirit of Charles Burchfield’s Summer Benediction (1948). While Adolph Gottlieb’s Untitled (1946) and Alexander Calder’s The Two Arrows (1966) explore abstract shapes and formal relationships, portraiture in watercolor ranges from the traditional—Thomas Eakins’s profile of an elderly woman seated in historicized surroundings in Seventy Years Ago (1877)—to the irreverent—Claes Oldenburg’s Blueberry Pie à la Mode, Tipped Up, and Spilling (1996).
Edward Hopper, Universalist Church, 1926. Watercolor over graphite on cream wove paper. Laura P. Hall Memorial CollectionThe works in the exhibition address broad artistic and historical trends while revealing the medium’s distinctive technical properties as an amalgam of painting and drawing. They also represent a wide range of subject matter and styles. Highlights include Winslow Homer’s Eastern Point Light (1880), an evocative portrayal of two ships, one brilliantly silhouetted by moonlight;Universalist Church (1926) by Edward Hopper, a dramatically cropped study of New England light on a historic church steeple and the structures that surround it; and Jacob Lawrence’s The Workshop (1978), whose signature flattened colors embody the artist’s modernist sensibility. Landscape plays a major role in the medium, as seen in such images as the dramatic mountain scene (ca. 1908) by John Singer Sargent, Arthur Dove’s interlocking Two Trees (1937), and the swirling forms and life-affirming spirit of Charles Burchfield’s Summer Benediction (1948). While Adolph Gottlieb’s Untitled (1946) and Alexander Calder’s The Two Arrows (1966) explore abstract shapes and formal relationships, portraiture in watercolor ranges from the traditional—Thomas Eakins’s profile of an elderly woman seated in historicized surroundings in Seventy Years Ago (1877)—to the irreverent—Claes Oldenburg’s Blueberry Pie à la Mode, Tipped Up, and Spilling (1996).